Many procedures listed below are minimally invasive and carried out
with either x-ray or ultrasound guidance. This improves the accuracy, safety, and comfort during the procedure. Some of the more common procedures we offer are listed below:
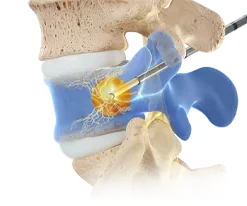
- Basivertebral nerve ablation (Intracept) ***NEW*** – ADDITIONAL INFORMATION
- Cervical epidural steroid injections – VIDEO
 Cervical medial branch blocks/facet joint injections – PATIENT EDUCATION HANDOUT
Cervical medial branch blocks/facet joint injections – PATIENT EDUCATION HANDOUT- Cervical radiofrequency ablation – VIDEO – PATIENT EDUCATION HANDOUT
- Thoracic epidural steroid injections
- Thoracic medial branch blocks/facet joint injections
- Thoracic radiofrequency ablation
- Kyphoplasty – PATIENT EDUCATION HANDOUT
- Lumbar Discography – VIDEO
- Lumbar epidural steroid injections – VIDEO
- Lumbar facet joint injection – VIDEO
- Lumbar medial branch blocks – VIDEO – PATIENT EDUCATION HANDOUT
- Lumbar radiofrequency ablation – VIDEO – PATIENT EDUCATION HANDOUT
- Lumbar selective nerve root/transforaminal epidural injections
- Sacroiliac joint injections – VIDEO – PATIENT EDUCATION HANDOUT
- Caudal epidural injections – an epidural injection performed near the tailbone area
- Sympathetic nerve blocks: Stellate ganglion, Lumbar sympathetic (VIDEO), and Ganglion impar blocks
- Peripheral nerve and joint injections with corticosteroid or hyaluronic acid, aka “lubricant”: Shoulders, hips, knees, etc…
- Spinal cord stimulation – VIDEO
- Genicular (Knee) blocks and radiofrequency ablation – PATIENT EDUCATION HANDOUT
- Peripheral nerve blocks for groin and testicular pain (ilioinguinal, iliohypogatric and pudendal nerve blocks)
- Trigger point injections – VIDEO
- Carpal tunnel injections
- Botox for the treatment of chronic migraine (a chronic migraine is defined as having a headache for more than 15 days per month and lasting more than 4 hours per day) – Click HERE for additional information
- Botox for the treatment of limb spasticity
- Occipital nerve blocks
- Note: Ultrasound guidance is commonly used for these injections to improve accurate delivery and effectiveness of the medicine. It also improves the comfort of the procedure